
How health status affects labour market participation


The health of the population is a key driver of the medium-term economic and fiscal outlook, and the costs of poor health pose one of the biggest risks to the long-term sustainability of the public finances. Our 2024 Fiscal risks and sustainability report explored these risks in the context of recent developments, including scenarios for the effects of population health on long-term economic and fiscal prospects.
A key channel for these effects was via the labour market, where we calibrated our scenarios by attempting to isolate the impact of health status on labour participation. This article presents this estimation in more detail. It also discusses how we interpret the results and their implications for our ongoing work on the interplay between health, health spending, and the economy and public finances.
Scenarios for the impact of better or worse health on the public finances

As well as a review of recent trends in health and health spending and an update to our baseline health spending projections, our 2024 Fiscal risks and sustainability report set out scenarios for better or worse outcomes for the health of the population over the next 50 years. These explored the implications of different health trajectories for the labour market, GDP, tax revenues, and government spending on health, welfare, and pensions.
The scenarios aimed to present plausible upper and lower estimates for how health trends could evolve over the next half century and what this could imply for the public finances (while remaining neutral on the policy and other drivers of these outcomes). They were conditioned on a 25 per cent deterioration or improvement in work-limiting ill health across age ranges over the next 50 years,1 broadly reflecting a reversal (in the better health scenario) or doubling (in the worse health scenario) of the trends observed over the past decade or so.2
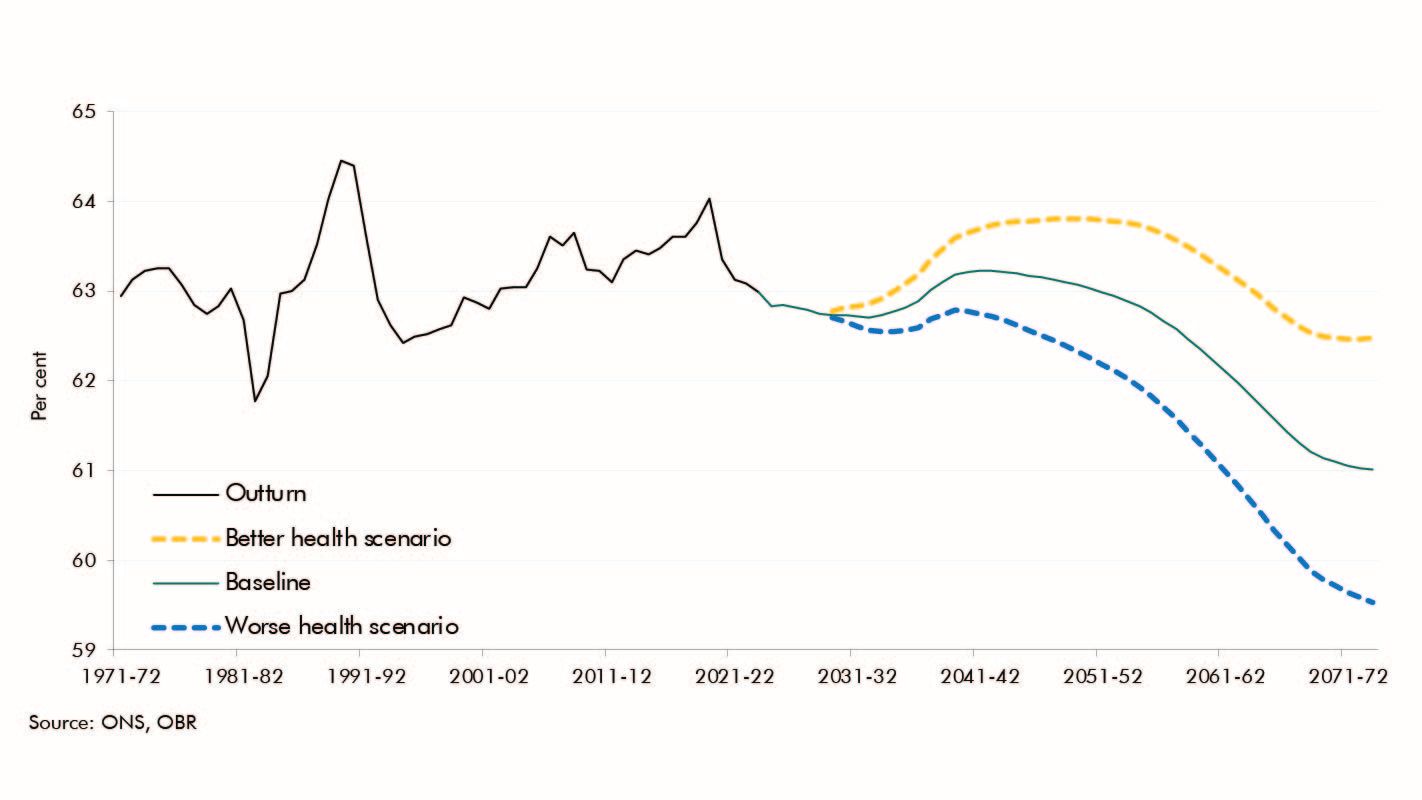
Our approach to understanding the impact of these health changes on tax revenues and welfare spending rested on converting them into the changes in labour market participation shown in the chart below. We did this by estimating a ‘health participation factor’ of 28 per cent, which represents the decrease in a person’s likelihood of being in the labour force at a given age if they switch from good health to ill health (the methodology we used to estimate this is discussed below).3 The result was a 1.5 percentage point increase or decrease in the participation rate in 2073-74 relative to the baseline, equivalent to around 1 million more or fewer people in the labour force.
16+ participation rate in the scenarios
Participation ends up around 1½ percentage points higher or lower in the better and worse health scenarios

We then translated these participation changes into changes in real GDP, assuming, in line with our previous analysis, that changes in participation occur at below-average hours and earnings. We also included equivalent changes in the health status of those remaining in work, with implications for their hours and earnings too. Combining these estimates resulted in real GDP being around 2½ per cent higher or lower in the better and worse health scenarios respectively by the 2070s.
The health participation factor – isolating the impact of health status on participation


People with health conditions have lower employment and participation rates. There’s also plenty of evidence that poor health is co-incident with many other factors that negatively influence labour market outcomes, including lower levels of education and lower income and wealth. So in estimating the ‘health participation factor’ we sought to ‘control’ for individual characteristics that have a large bearing on participation, in order to zoom in more precisely on the impact of health status.
We did this by running a logistic regression (and marginal probabilities on its basis) using Labour Force Survey (LFS) data, with labour market participation as the dependent variable and the presence of a work-limiting health condition as an independent variable, alongside highest qualification, age, homeownership status and gender:
Labour market participation = α+β0 health condition + β1qualification + β2age + β3homeownership + β4gender + ε
The results of this regression (the marginal probabilities in the final column of the table below) show that controlling for these factors, the presence of a self-reported, work-limiting health condition is estimated to reduce an individual’s chances of participating by 27.5 per cent. This is slightly larger than the effects of age group, for which the ‘reference category’ is those aged 16-24, so the results in the final column of the table below suggest that being aged 35-49 is associated with a 24.3 per cent increase in the likelihood of participating relative to being 16-24. And the presence of a work-limiting health condition appears comfortably more important for participation than qualification level, homeownership or gender.4Our approach is a relatively simple specification with limited covariates (meaning it is likely an upper estimate) for the purpose of constructing broad scenarios, and so by no means the definitive word on the importance of health status for participation relative to other factors.5 But the results are nonetheless useful.
Results of logistic regression on labour market participation
|
Coefficient1 |
Odds ratio2 |
Probability of participation for given characteristic3 Per cent |
Marginal probability of participation for given characteristic4 |
|
|---|---|---|---|---|
|
Work-limiting health condition |
-1.6 *** |
0.2 |
16.1 |
-27.5 |
|
Highest qualification (compared to 'no or below GCSE' qualifications) |
||||
|
.....GCSE or A-level equivalent |
0.6 *** |
1.9 |
65.1 |
9.7 |
|
.....Degree equivalent or above |
1.2 *** |
3.2 |
76.0 |
16.2 |
|
Age (compared to age 16-24) |
||||
|
.....25-34 |
1.6 *** |
5.0 |
83.3 |
24.1 |
|
.....35-49 |
1.6 *** |
5.1 |
83.6 |
24.3 |
|
.....50-54 |
1.5 *** |
4.3 |
81.2 |
22.6 |
|
.....55-59 |
0.9 *** |
2.5 |
71.6 |
15.8 |
|
.....60-64 |
-0.1 |
0.9 |
48.4 |
-1.3 |
|
Homeowner |
0.5 *** |
1.6 |
61.7 |
6.4 |
|
Female |
-0.5 *** |
0.6 |
37.4 |
-6.7 |
|
Constant |
0.1 *** |
1.1 |
52.0 |
|
|
1Coefficients in logistic regressions do not themselves have direct real-world interpretations - see subsequent columns for interpretation. Statistical significance at the 1 per cent confidence level indicated by ***. Note: Based on 2022 data (pooled LFS quarters) for 16-64 year olds. Source: ONS, OBR |
||||
Conclusions and implications


As well as helping us to set out economic and fiscal scenarios for the impact of better or worse health outcomes, this analysis has implications across different aspects of the OBR’s work.
First, it suggests that health status is likely one of the most important factors in determining labour market outcomes, alongside things like age and qualification level that are more often front of mind. That health is important may not be a surprise to anyone familiar with recent trends in economic inactivity or welfare spending. But these results serve as a useful reminder of the range of contextual factors that we should consider when putting together our labour market and welfare forecasts (as we concluded for the latter in our recent Welfare trends report).
Second, while health is important, it’s probably wrong to assume that even transformative improvements in people’s health have anything like as large (in terms of the number of people affected) effects on economic activity. Put crudely, if we assume our estimates work in both directions, they imply that there is only a 28 per cent chance that working-age people in ill health who get better (or who are prevented from becoming ill) will move into (stay in) the labour force, relative to if they remained in or moved into in ill health. This is consistent with our previous modelling of the impact of reducing the NHS waiting list on economic activity, and underscores the need for a strong evidence base in order to incorporate the economic effects of health interventions in our economy forecasts.
Finally, although this analysis has focused on the impact of health on labour market outcomes, the relationship is in reality two-way, with work generally good for health and wellbeing. There will also be interdependencies between health and other factors discussed here, like educational attainment and wealth. Delving further into these ‘virtuous’ or ‘vicious’ cycles of health and economic outcomes is something we will consider for future work in this area.
Acknowledgements
We are grateful for the engagement, expertise, and insights from various OBR staff members in compiling this article, in particular Joshua Rawlings.
Downloads
How health status affects labour market participation (article PDF)